
Spinal Cord Injuries
Our Male Infertility Specialist:
It is well established that fertility in many paraplegic and quadriplegic men after spinal cord injuries is severely impaired. The two major causes of infertility of men with Spinal Cord injuries (SCI) are ejaculatory dysfunction and poor semen quality.
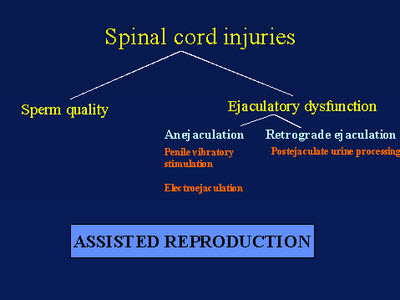
In addition to poor sperm quality, ejaculatory dysfunction is a major cause of infertility on men with SCI. Two types of ejaculatory dysfunction are anejaculation and retrograde ejaculation.
Retrograde ejaculation occurs when the bladder neck region does not close properly during emission. The diagnosis of retrograde ejaculation is confirmed by the presence of sperm in the postejaculate urine analysis (PEU). Sperm concentration and motility are determined in the specimen. If concentration is adequate and motility is poor, urine must be alkalinized with oral medications ( sodium bicarbonate) to pH 7.5-8.0 for optimal sperm survival. Patient is instructed to void without complete emptying of the bladder, immediately ejaculate and urinate again into a specimen cup containing culture media. Occasionally sperm processing media is instilled after patient voided and before ejaculation. The urine-sperm mixture then processed for sperm recovery, which could be used for intrauterine insemination or other assisted reproductive techniques. In the past sperm has been retrieved from men with SCI by a variety of methods including intrathecal and subcutaneous administration of cholinesterase inhibitors and surgical extraction of sperm from the vas deferens. Because of potential adverse effects from cholinesterase inhibitors, such as paroxysmal changes in blood pressure, these procedures have become less commonly used in clinical practice. Vasal sperm retrieval potentially may cause scarring and obstruction of vas deferens and epididymis. Penile vibratory stimulation and electroejaculation are the most popular current methods of obtaining sperm specimen for the purpose of fertility.
The aim of Penile vibratory Stimulation(PVS) is to activate normal ejaculatory reflex. The vibrating probe held against frenulum activates an afferent stimulus. Penile erection usually but not necessarily occurs. Periurethral contraction then proceed in a rhythmic fashion with antegrade ejaculation. If PVS is not successful, it may be repeated up to 6 times with 1-2 min. interval before categorized as a PVS failure. The level of spinal cord injury has significant prognostic value with the higher lesion (>T9) and intact reflexes below the level of SCI showing significantly higher success rate.
Although the ejaculation from PVS ranges from 24-91% by using optimized vibration parameters, sperm quality is poor among responders. Sperm count may be quite high but motility is low.
Complication rate is quite low. Skin swelling and abrasions are usually mild. Autonomic dysreflexia with severe elevation of blood pressure occasionally observed in men with lesions above T6. This patient should receive prophylactic nifedipine 10-20 mg SL 10 minutes before the procedure.
The ultimate goal of PVS is to be performed in the outpatient setting by teaching the couple to achieve pregnancy by their own using vaginal self-insemination. If sperm quality is poor and no pregnancy occurred, more vigorous treatment can be employed (IUI, IVF, and ICSI)
PVS may be considered as a first line of treatment of anejaculation in patients with SCI due to its safety, relative effectiveness, and low cost.
Rectal Probe ejaculation (Electroejaculation-EE)
If PVS is not successful, EE can be employed. It is routinely successful in obtaining sperm and has high success rate in all types of SCI.
The procedure is performed in the OR under general anesthesia. Bladder is catheterized and filled up with 30-40 cc of HTF buffer solution. After catheter is removed the patient is placed in the lithotomy position. Anoscopy is performed to exclude possible rectal mucosal lesions. Then rectal probe of Seager Electroejaculator is inserted to its hub with electrode facing anteriorly toward the prostate and seminal vesicles. Pulsatile stimulation begins to a maximum voltage of 20 and current density up to 400 mA for up to 3 sec per stimulation The probe thermistor monitored temperature should not rise above 39 C. After antegrade ejaculation semen collected in the sterile wide mouth cup, rectal probe removed and repeat anoscopy is performed. Bladder catheterized and possible retrograde specimen is collected. Both specimens are processed in the andrology lab for future use in the insemination protocol/IVF etc.
Complications from EE include autonomic dysreflexia and rectal injury
Assisted ejaculation methods can produce samples in 75-100% of patients with spinal cord injury. However, the majority of these patients have poor sperm quality characterized with low motility, abnormal morphology and increased number of WBC in the ejaculate. Unfortunately, exact cause of these sperm abnormalities are not known. Possible causes of poor sperm quality after SCA include stasis of prostatic fluid, testicular hyperthermia, urinary tract infection, type of bladder management, abnormal testicular histology, sperm contact with the urine, possible changes in hypothalamo-pituitary-testicular axis, possible sperm antibodies and long-term use of various medications. Recently higher level of reactive oxygen species in sperm of men with spinal cord injuries was documented.
As a result, cumulative natural pregnancy rates are low. In order to improve pregnancy and delivery rates, it is necessary to utilize assisted reproductive technologies. The delivery rates after IUI with stimulated cycle are within 10-13%. With IVF/ICSI the fertilization rate of 44-88% have been achieved.
In case of severe ejaculatory disorders and unsuccessful assisted ejaculation, sperm could be retrieved from the vas deferens, epididymis or testis and used for IVF/ICSI.